
Shoulder Pain With Full ROM: Rotator Cuff Tendinosis, Scapular Control, and the Low-Back Connection
ABSTRACT
Rotator cuff tendinosis and biceps tendonitis can hurt even with a full range of motion. Learn how scapular dyskinesis, trunk control, and thoracolumbar fascia load transfer can connect shoulder pain (45–75° arc) to low-back symptoms after lumbar fusion—and what a regional interdependence rehab plan looks like.
Key Topics
rotator cuff tendinosis
biceps tendonitis shoulder pain
shoulder pain with overhead lifting
shoulder pain 45 to 75 degrees
rotator cuff tendinopathy rehab
scapular dyskinesis and shoulder pain
scapular mechanics trunk stability
thoracic spine and shoulder function
regional interdependence shoulder and low back
thoracolumbar fascia function
shoulder pain after lumbar fusion
thoracolumbar fascia load transfer arms and legs
shoulder pain with light load mid-range
trunk control exercises for shoulder pain
low back pain triggered by arm loading
shoulder rehab Denver
personal trainer shoulder pain Denver
rotator cuff rehab Denver
Don’t let this type of shoulder discomfort take you away from your personal training sessions in Denver……but don’t ignore it either.
client injury
You received the following diagnosis after a review of her MRI findings: "MRI reviewed shows rotator cuff tendinosis, no full-thickness tear identified. Biceps tendonitis. AC arthrosis. Intact GH cartilage. left rotator cuff tendinosis and biceps tendonitis." Despite this diagnosis, you have a full range of motion on frontal and lateral raises. You feel discomfort, though, when the shoulder raise is loaded through the 45 to 75 degree phase of the movement with a light load. Other considerations include your lower back. You had a spinal fusion about two years ago and have chronic pain in the lower left lumbar region. When you perform a single-leg squat on your left leg while raising and extending both arms in front, you experience discomfort in your left serratus and in the areas of your serratus posterior inferior and iliocostalis lumborum. When placing your left foot in front of your right foot on a line, you feel a stretch in your left oblique. In contrast, you don't feel the oblique while stepping one foot in front of the other on a line, but tend to drop your left shoulder when the left foot is placed in front of the right foot on the line. Also, you unconsciously externally rotate your left foot while exercising on the Helix Lateral Elliptical.
The Assessment
Our working theory for right now: Your shoulder and lower back are connected through the muscles and connective tissue that transfer force between your arms and legs. Because your lower back had to adapt after surgery, your body now relies more on specific muscles and tissues on the left side to stabilize you. When you load your arms—especially in specific ranges—those tissues get overworked, which irritates both your shoulder and your lower back. The goal isn’t just to strengthen your shoulder or protect your back, but to help your whole system share the load more evenly again. Here's a more technical breakdown:
1. The shoulder does not function independently of the trunk
The shoulder complex depends on a stable yet adaptable base formed by:
the thoracic spine,
the rib cage,
the scapulae,
and the thoracolumbar fascia.
In your case:
Your left shoulder pain is provoked under load, not by range alone.
Your left lumbar region becomes symptomatic during arm-loaded single-leg tasks.
This indicates a load-transfer problem, not simply a local tissue problem.
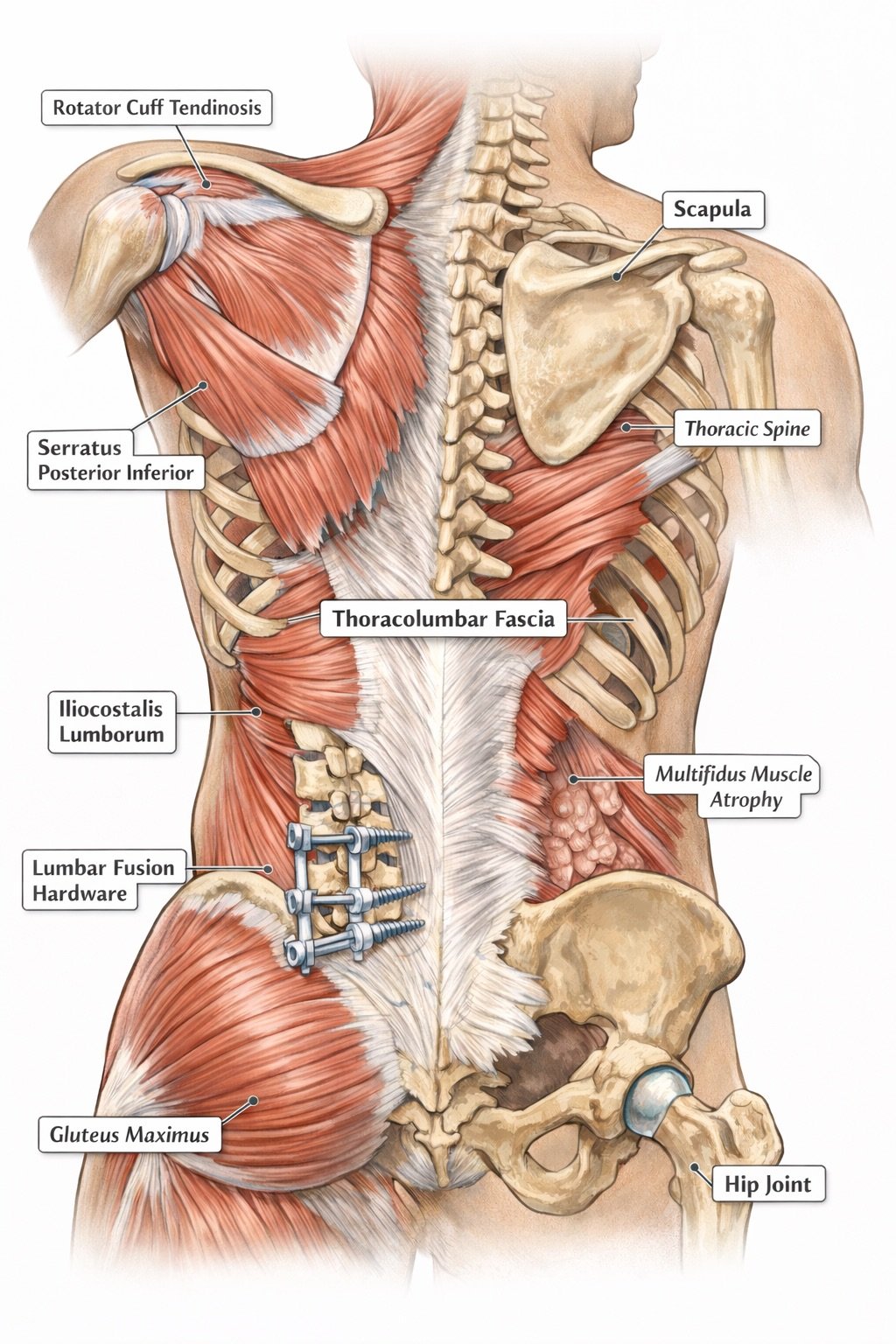
2. The thoracolumbar fascia is the key connector
The thoracolumbar fascia (TLF) is a dense connective tissue system that:
connects the latissimus dorsi, serratus posterior inferior, obliques, multifidi, and gluteus maximus,
transmits force between the upper limb and lower limb,
provides passive stiffness and proprioceptive input during movement.
Why this matters for You
Your discomfort localizes near the left paraspinal incision and lateral lumbar musculature.
You report discomfort in the serratus posterior inferior / iliocostalis region during arm-loaded, single-leg tasks.
These structures are directly integrated through the TLF.
When you raise your arms—especially under load—the demand for force transmission through this fascial system increases. If one link is compromised, stress is shifted elsewhere.
3. Lumbar fusion alters load-sharing and motor control
Following an L4–5 fusion:
Segmental motion is intentionally eliminated.
Adjacent musculature and fascial tissues must absorb and redirect forces that were previously distributed across spinal motion segments.
Deep stabilizers (e.g., multifidi) often show atrophy or delayed activation, as your MRI has already documented.
Clinical consequence:
When you perform tasks requiring trunk stiffness (single-leg stance, arm elevation, reaching), you likely rely more on:
lateral trunk musculature,
thoracolumbar fascia tensioning,
and rib-scapular strategies.
This increases local tissue strain near the left hardware region and the lateral lumbar fascia.
4. How this feeds directly into your shoulder symptoms
Scapular mechanics depend on trunk control
Efficient shoulder elevation requires:
thoracic extension and rotation,
rib cage control,
coordinated serratus anterior and lower trapezius activity.
If the trunk is:
guarding,
asymmetrically stiff,
or over-recruiting lateral stabilizers,
then the scapula:
upwardly rotates less efficiently,
posteriorly tilts less,
and places greater compressive demand on the rotator cuff and biceps tendon—especially in the 45–75° mid-range, exactly where you report discomfort.
This explains an important clinical paradox
You have:
full shoulder ROM,
good isolated strength,
yet pain with light loading in a specific arc.
That pattern is classic for proximal control failure, not primary shoulder weakness.
5. Your observed compensations support this model
Each of your observations reinforces the same system-level explanation:
A. Single-leg squat (left) plus arms straight forward leads to left lumbar/serratus discomfort
This task dramatically increases:
anti-rotation demand,
lateral trunk stiffness demand,
force transfer through the thoracolumbar fascia.
Your system responds by overloading the left lateral trunk instead of distributing the load.
B. Tandem stance with left foot forward leads to the left shoulder drop
Indicates difficulty maintaining lateral trunk and scapular alignment on the left.
The shoulder drop is a compensation to reduce trunk demand.
C. Left foot external rotation on the Helix
A distal strategy to create stability when proximal control is limited.
Often seen when the system is avoiding the demand for hip/trunk internal rotation.
These are not random habits; they are protective motor strategies.
6. Why treating only the shoulder (or only the back) is insufficient
If treatment focuses solely on:
Rotator cuff strengthening without addressing trunk control is likely to result in recurrent shoulder symptoms.
Lumbar pain without integrating upper-quarter load transfer, daily activities (reaching, lifting, swimming) will continue to provoke symptoms.
Your condition requires a regional interdependence approach:
shoulder loading tolerance,
scapular mechanics,
trunk stiffness and endurance,
hip contribution,
and graded re-exposure to integrated patterns.
Research-Based Citations
Yang Y, Wu Y, Zhang H, Zhang J, Li J, Li S, et al. (2025). An additional rehabilitation program to improve postoperative outcomes in patients with rotator cuff tears and scapular dyskinesis: a propensity score-matched study. BMC Musculoskeletal Disorders.
PMID: 40188115
DOI: 10.1186/s12891-025-08596-x
Vining R, Onifer SM, Twist E, Ziegler AM, Corber L, Long CR. (2023). Thoracolumbar fascia mobility and chronic low back pain: Phase 1 of a pilot and feasibility study. Journal of Bodywork and Movement Therapies.
PMID: 37301552
DOI: 10.1016/j.jbmt.2023.04.004
Lin GX, Ma YM, Xiao YC, Xiang D, Luo JX, Zhang GW, Ji ZS, Lin HS. (2021). The effect of posterior lumbar dynamic fixation and intervertebral fusion on paraspinal muscles. BMC Musculoskeletal Disorders.
PMID: 34930199
DOI: 10.1186/s12891-021-04943-w
PubMed: https://pubmed.ncbi.nlm.nih.gov/34930199/
Frequently Asked Questions (FAQs)
1) What is rotator cuff tendinosis (tendinopathy)?
Rotator cuff tendinosis is a chronic overload/degeneration pattern in the tendon (often without a full-thickness tear). Symptoms frequently show up with loading and repetition more than with the range of motion alone.
2) Why can I have full shoulder range of motion but still feel pain when lifting?
A full ROM with pain during a specific loaded arc often suggests a load-management and control issue—how force is transferred and distributed—rather than a simple “you’re weak” problem.
3) Why does shoulder pain commonly show up between ~45–75 degrees of elevation?
Mid-range elevation can increase compressive demand on the rotator cuff and biceps tendon—especially if scapular upward rotation/posterior tilt and trunk mechanics are not coordinating efficiently.
4) What is scapular dyskinesis, and why does it matter here?
Scapular dyskinesis is an alteration in scapular position or movement. If the scapula does not rotate upward or posteriorly tilt well, the shoulder may “borrow” stability from the rotator cuff and biceps tendon during elevation, increasing the risk of irritation.
5) How could a lumbar fusion influence shoulder symptoms?
After fusion, the system has fewer motion segments to share load, and paraspinal muscles can demonstrate atrophy/degenerative changes. That can shift stabilization strategies during reaching and lifting—especially in single-leg or anti-rotation tasks—contributing to overload elsewhere.
6) What does the thoracolumbar fascia have to do with shoulder and low-back pain?
The thoracolumbar fascia is a layered connective-tissue system involved in trunk stiffness and load transfer. Research using imaging approaches suggests altered mechanics of the thoracolumbar fascia (e.g., reduced shear strain/mobility) in chronic low-back pain populations.
7) What is a “regional interdependence” rehab approach?
It means you train the painful area (shoulder) and the regions that feed it (thorax/rib cage, trunk, hips) so the whole system shares load more evenly during real tasks like lifting, reaching, and single-leg stability.
8) What types of exercises usually fit this presentation?
Common categories include: scapular control (serratus anterior/lower trap bias), thoracic mobility/extension tolerance, trunk endurance (anti-rotation/anti-extension), hip contribution (especially single-leg stability), and graded re-loading of the painful arc.
9) When should I get medical evaluation vs. self-manage?
Seek evaluation promptly if you have significant night pain, rapidly worsening weakness, neurological symptoms, fever/unexplained swelling, or loss of function after a traumatic event. Otherwise, a progressive loading plan guided by symptoms and function is often appropriate.
ABOUT THE AUTHOR: MICHAEL MOODY, PERSONAL TRAINER
As an author, a personal trainer in Denver, and podcast host, Michael Moody has helped personal training clients achieve new fitness heights and incredible weight loss transformations since 2005. He also produces the wellness podcast "The Elements of Being" and has been featured on NBC, WGN Radio, and PBS.
Michael offers personal training to Denver residents who want to meet at the 2460 W 26th Ave studio….or in their homes throughout LoHi (80206), LoDo (80202), RiNo (80216), Washington Park (80209), Cherry Creek (80206, 80209, 80243, 80246, 80231), and Highlands (80202, 80211, 80212). Michael also offers experiences with a personal trainer in Jefferson Park (80211) and Sloan's Lake (80204, 80212).
If you’re looking for a personal trainer who can curate a sustainable (and adaptable) routine based on your needs and wants, Michael is the experienced practitioner you’ve been looking for. Try personal training for a month…your body will thank you!





























